by Thomas Lethenborg | Aug 21, 2020 | News
Quality Policy and Standards
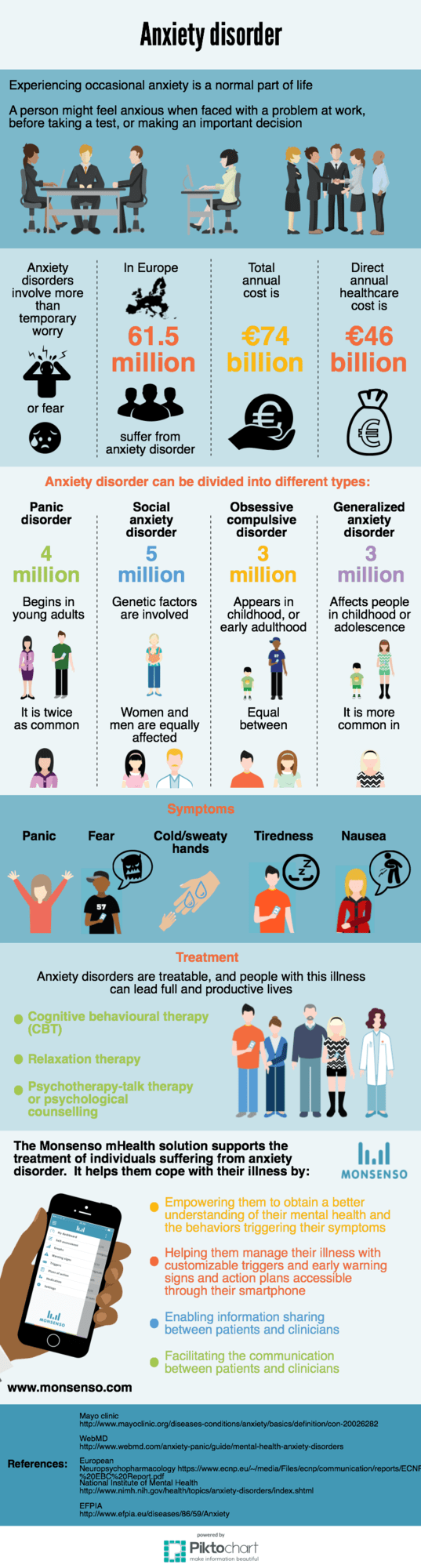
As a technology leader in mobile health (mHealth) solutions for mental health, Monsenso is ISO 13485 certified.
ISO 13485 is the gold standard for medical device companies to ensure the quality, safety and efficacy of products in the medical device field. This certification ensures that the product in question, consistently meets customer requirements and regulatory requirements applicable to medical devices and other related services.
“Monsenso adheres to the highest security standards. Beyond, being ISO 13485, Monsenso holds the ISO 27001 certifications, a TGA certification and class 1 CE mark.” says Thomas Lethenborg, CEO at Monsenso.
You can download this article as PDF in English.
For additional information contact:
Bettina van Wylich
Chief Marketing Officer
Monsenso
+45 22704724
wylich-muxoll@monsenso.com

by Thomas Lethenborg | Aug 21, 2020 | News, Press releases
Quality Policy and Standards
As a technology leader in mobile health (mHealth) solutions for mental health, Monsenso is ISO 13485 certified. ISO 13485 is the gold standard for medical device companies to ensure the quality, safety and efficacy of products in the medical device field. This certification ensures that the product in question, consistently meets customer requirements and regulatory requirements applicable to medical devices and other related services.
“Monsenso adheres to the highest security standards. Beyond, being ISO 13485 certified, Monsenso holds the ISO 27001 certification and class 1 CE mark.” says Thomas Lethenborg, CEO at Monsenso.

For additional information contact:
Jennifer Highland
Marketing and Communications Manager
Monsenso
+45 81 71 7713
highland@monsenso.com

by Thomas Lethenborg | Jun 21, 2016 | Blog, Mental Illness, mHealth
According to a recent statement by the new American Heart Association (AHA), major depressive disorder and bipolar disorder should be recognized as moderate risk factors for atherosclerosis and early cardiovascular disease. [1]
In 2011, the National Heart, Lung and Blood Institute identified four conditions (chronic inflammatory disease, human immunodeficiency virus, Kawasaki disease, and nephritic syndrome) that lead youths to a mild risk of developing cardiovascular disease before they reach 30. [2]
The statement released a few days ago, reveals that depression and bipolar disorder meet the same criteria as these conditions. Moreover, these two behavioural disorders are more widespread than the previous mentioned conditions combined.
These studies showed evidence of a link between paediatric depression and bipolar disorder with premature cardiovascular mortality. Cardiovascular risk factors for these teens include obesity, insulin resistance and diabetes, dyslipidemia, and hypertension.[1] According to the statement, depression and bipolar disorder are the first- and fourth-most disabling conditions, among adolescents worldwide.
After the report had been unveiled, researchers from schools around the U.S. and Canada looked at existing studies on mood disorders in people under the age of 30. Researchers looked specifically into youths suffering from depression or bipolar disorder with cardiovascular markers such as high pressure and cholesterol. They found a significant connection between having depression or bipolar disorder and increased odds of high blood pressure, high cholesterol, obesity (especially belly fat), type 2 diabetes, and hardening of the arteries. [3]
This discovery denotes that healthcare providers should track physical activity levels and food intake as well as metabolic monitoring is crucial for these young patients as a preventive measure.
However, to monitor cardiovascular markers, physical activity and food intake, of thousands of young patients who also suffer from mental illness is not an easy task. Although, there are hundreds of smartphone applications tracking physical activity and counting calories, these apps are personal, and clinicians do not have access to an individual’s data. Nevertheless, with the Monsenso mobile health (mHealth) solution, this cumbersome task becomes easy and achievable.
The Monsenso mHealth solution enables clinicians to access a patient’s data on a daily basis. Every day, youths would be reminded to fill in a self-assessment with important information that could include the number of hours they slept, the amount of unhealthy food they have eaten, and if they realized any physical activity throughout their day. Additionally, the smartphone can also collect physical activity and mobility data, based on the smartphone’s inbuilt accelerometer and GPS locator.
The Monsenso mHealth solution, especially designed to monitor behavioural data of patients suffering from mental illness, can in this way help clinicians monitor any unhealthy habits of patients with risk of developing cardiovascular disease.
Further, with the customisable action plans, each youth could follow “contingency plans” if they experience some symptoms related to their mental illness or if they have engaged in unhealthy activities. For example, a special trigger could set up if a youth has indulged in unhealthy food for several days in a row, or has had a low level of physical activity. The action plan listed for this trigger could then encourage individuals to engage in physical activities and and to try to avoid sugar and fat during the upcoming week.
References:
[1] Browser,D Medscape. Depression, Bipolar Disorder in Teens are CVD Risk Factors: AHA (2015, August 10) http://www.medscape.com/viewarticle/849312
[2] American Heart Association. Young people with mood disorders have increased risk of developing early cardiovascular disease (2015, August 11)
http://blog.heart.org/young-people-with-mood-disorders-have-increased-risk-of-developing-early-cardiovascular-disease/
[3] Walton, A Forbes. Teens with depression, bipolar disorder, should be screened for heart disease, experts say. (2015, August 11) http://www.forbes.com/sites/alicegwalton/2015/08/11/depressed-teens-may-be-at-higher-risk-for-heart-disease/
Goldstein BI, Carnethon MR, Matthews KA, et al. Major depressive disorder and bipolar disorder predispose youth to accelerated atherosclerosis and early cardiovascular disease. Circulation 2015.

by Thomas Lethenborg | Dec 8, 2015 | mHealth
Early intervention is critical to treating mental illness before it can cause tragic results such as serious impairment, unemployment, homelessness, poverty, and suicide [1].
The identification of mental illness and its treatment, as early as possible, represents a high priority. The early detection and treatment of mental illness promote recovery, independence, and self-sufficiency, as well as facilitating social activities and employment opportunities [2].
It is estimated that 100,000 adolescents and young adults in the United States alone experience a first episode of psychosis every year. The early phase of psychotic illness is widely viewed as a critical opportunity for indicated prevention, and a chance to alter the downward trajectory and poor outcomes associated with serious mental disorders such as schizophrenia. The timing of treatment is critical; short and long-term outcomes are better when individuals begin treatment close to the onset of psychosis. Numerous studies find a substantial delay between the onset of psychotic symptoms and the initiation of treatment. In the U.S., treatment is typically delayed between one and three years, suggesting that many people experiencing first episodes of psychosis are missing a critical opportunity to benefit from early intervention [3].
Early identification and rapid referral are essential to shortening the duration of untreated psychosis and pre-empting functional deterioration. The World Health Organization advocates reducing the duration of untreated psychosis to three months or less by addressing “bottlenecks” in the pathway from early psychosis identification to initiation of specialty care [3].
To support early intervention, in 2009, the National Institute of Mental Health (NIMH), implemented a research project to change the prognosis of schizophrenia through aggressive treatment in the earliest stages of illness.Recovery After an Initial Schizophrenia Episode (RAISE) is designed to reduce the likelihood of long-term disability that people with schizophrenia often experience. It aims to help people with the disorder lead productive, independent lives. At the same time, it aims to reduce the financial impact on the public systems often tapped to pay for the care of people with schizophrenia [4].
In 2011, RAISE began conducting a full-scale, randomized controlled trial comparing two different ways of providing treatment to people experiencing the early stages of schizophrenia and related disorders. Both types of treatment emphasize early intervention but feature different approaches for initiating and coordinating care. Treatment may include personalized medication treatment, individual resiliency training, and supportive services, such as family psychoeducation and education or employment assistance [5]. The RAISE study, expected to be completed by August 2016, aims to emphasize the importance of early intervention.
The Monsenso mHealth solution can help healthcare providers to closely monitor patients who have experienced a first episode of mental illness.
After experiencing a first episode, the healthcare provider can encourage the patient to use the Monsenso mHealth solution. This will enable the clinician to monitor the individual on a continuous basis, and react if symptoms arise.
With the Monsenso user app, patients can fill in self-assessments on a daily basis. These self-assessments include information on the patient’s behaviour and symptoms related to his mental health. Furthermore, the solution collects sensor data through sensors in the patient’s smartphone, and this combined with the self-assessment will help the healthcare provider to continuously monitor the patient, and support intervention at a very early stage. Early warning signs and automatic triggers can be set to indicate to the health care provider that proactive intervention is needed, if for example a patient sleeps too little or feels too distressed.
Early intervention and continuous monitoring can maximize a person’s chances of a fast recovery, self-sufficiency, and living a high-quality life including the possibility to pursue and education and maintain a stable job.
References:
[1] Directors Blog: SAMHSA and NIMH partner to support early intervention for serious mental illness. P. Hyde and T. Insel. National Institute of Mental Health Blog (2014, June 17) http://www.nimh.nih.gov/about/director/2014/samhsa-and-nimh-partner-to-support-early-intervention-for-serious-mental-illness.shtml
[2] Early intervention and recovery for young people with early psychosis: consensus statement. J. Bertolote and P. McGorry. British Journal of Psychiatry (2005). http://bjp.rcpsych.org/content/bjprcpsych/187/48/s116.full.pdf
[3] Evidence based treatment for first episode of psychosis: Components of coordinated specialty care. PHD R. K. Heinssen. RAISE NIMH (2014, April 14). http://www.nimh.nih.gov/health/topics/schizophrenia/raise/nimh-white-paper-csc-for-fep_147096.pdf
[4] Raise Project Overview. National Institute of Mental Health. (2009)http://www.nimh.nih.gov/health/topics/schizophrenia/raise/index.shtml
[5] NIMH RAISE Project makes progress as team refines research approach. National Institute of Mental Health. (2011, August 9) http://www.nimh.nih.gov/news/science-news/2011/nimh-raise-project-makes-progress-as-teams-refine-research-approaches.shtml