To turn on English subtitles, click on the ‘CC’ at the bottom of the video.
Psychiatrist Kristoffer Södersten from PsykiatriResurs in Sweden shares his experience using the Monsenso mHealth solution.
How does the Monsenso mHealth solution encourage and empower better mental health treatment?
Kristoffer explains how the Monsenso mHealth solution helps him to enhance and inform treatment. Specifically, the solution helps him to gain more relevant information about his patients, such as information that couldn’t have been obtained through the traditional method of verbal sessions. “It’s difficult to retrieve reliable and consistent data from each patient during a verbal consultation with them,” says Kristoffer.
Obtaining the right information is key for psychiatrists and psychologists to provide an accurate diagnosis
“[The accuracy from a diagnosis obtained] from face-to-face consultation depends so much on factors like personal relations, how comfortable the patient is in the conversation, cultural background, etc. Therefore, [due to these factors] it can be very arbitrary about which diagnosis a patient receives. This diagnosis can depend on which clinician he meets, and these other factors.” says Kristoffer. The information gathered from the Monsenso Clinic can help to provide a consistent and clearer view of the patient’s mental health, to better inform a diagnosis.
Kristoffer finds the Monsenso mHealth solution to be particularly helpful in capturing relevant objective data. The solution provides a comprehensive and easily accessible overview of relevant patient data, such as day score, mood score, sleep and medication adherence. Moreover, overview of collected sensor data, such as physical activity, social activity, phone usage and voice features can also be provided. This objective data can help to supplement the subjective data provided during verbal therapy.
“The technology of Monsenso can help us to gather more objective data that – together with the subjective experience – provide a more holistic picture of the patient’s problems, to help provide a more accurate diagnosis and follow-up treatment in a totally different way,” says Kristoffer.
Monsenso mHealth solution is providing a visualization of a historical data, which in some cases can identify why the symptoms appear and help to prevent them.
“You can also use this tool to predict future psychological outcomes, which can help us intervene early and prevent relapse.”
Like many Americans, I have a family member with a major mental illness who sometimes needs inpatient hospital care. Because I have been a healthcare researcher and journalist for 25 years, I’m particularly well prepared to help him navigate the system and get him the attention he deserves.
But there’s one issue which crops up again and again, and despite decades of trying I haven’t been able to find any kind of remedy. And as far as I can tell, this policy — which is universal in my region — actually encourages the delivery of substandard care.
As many people are aware, there’s far too few inpatient mental health beds in many regions of the country. My sense is that the problem may be a bit less acute where I live, in metro DC, as my relative can generally find inpatient care when he needs it. But which bed in which hospital? That’s another story.
Like any other service, inpatient mental health treatment can vary substantially from one institution to another. And as a member of a family support group for mental health problems, I get lots of feedback on which psych units are well-staffed, clean, efficient, thorough, kind to patients and good with discharge planning. (Of course, I also have my relative’s feedback and my own impressions to refer to as well.)
However, area hospitals with psych units absolutely, categorically refuse to tell patients or their families whether a bed is available. Yes, they will typically tell a psychiatrist with admitting privileges whether they can take additional patients, but for reasons which are not clear to me, a shrinking number of psychiatrists choose to obtain such privileges. In fact, in many years of trying, my relative hasn’t found a single one who does do direct admissions.
So here’s what happens. Our family realizes that he needs help, so one of us takes him to a hospital where he feels comfortable and safe. That hospital puts him through several hours of “medical clearance,” and only then do they let us know that there are no open beds there. Then they try to convince us to take whatever bed is available anywhere they can find.
In the most recent case, they pressured us to send him to Hospital X, an underfunded, poorly-rated facility which I’d dearly love to see decertified and closed. Since his episode seemed to be tailing off, we decided to take him home and bring him to another good facility the next day, which we did, successfully. But given the coercive nature of the original facility’s approach, it took all of the strength we could muster to do so.
I am certainly aware that with the limited availability of psych beds, every hospital will turn patients away at times. But if the hospitals let patients and/or family members know whether there was even a chance of admission, patients could make informed choices. They could also choose between their preferred hospitals, rather than being side-tracked into those that did not deserve their patronage.
My guess is that such hospitals, whose psych units are often unprofitable, are colluding to make sure that the more effective, humane and resource-rich psych units don’t get all of the traffic. After all, if patients don’t know which units can serve them, it’s easier for facilities to ricochet them across the region and give some of the inpatient days to whichever player is next in line.
But even if there’s no conspiracy involved, the policy of keeping patients out of the loop is unconscionable nonetheless. If patients end up wherever they’re sent, hospitals have no incentive to offer improved services. And that just about defines “anti-competitive.” I dearly hope someone calls these hospitals to account someday.
Monsenso, mHealth for mental health helps optimise the treatment of most major mental illnesses such as bipolar disorder, schizophrenia, borderline, depression, anxiety and PTSD.
Borderline personality disorder (BPD) is a severe mental illness that causes unstable moods, behaviour, and relationships. It usually begins during adolescence or early adulthood [1].
Most psychiatric disorders cause a permanent abnormal social behaviour, whereas borderline personality disorder only causes brief psychotic episodes. As a result, experts believe this is an atypical mental illness that can be misleading [2].
According to a 2015 study undertaken by French psychiatrist Lionel Cailhol, BPD is equally common in both genders. Nonetheless, in clinical populations, females represent 75% of all patients. Some experts believe this is due to men having difficulty seeking help, especially in psychotherapy [3].
BPD usually appears during late adolescence. However, clinicians recommend that a diagnosis should not be made before the age of 18 years. Patients should be treated later on when the symptoms are clear and persistent.
The most common causes of BPD are believed to be early maternal separation and childhood trauma [3]. However, identifying symptoms at an early stage or educating a child in a manner that could prevent BPD would spare the patient a lot of pain, time and money. As life-coach Tami Green explains in one of her talks, a good way of avoiding BPD is to accept people and their flaws without trying to change them. She gives an example of a very sensitive child that is pressured by their parents to become tougher and bearable, however the pressure violates this child to the core of who they are. It can be very difficult to handle this sort of conversation without criticizing them. [4]
It is particularly hard for families of adolescents, because they need to help their children cope with their behaviour, provide them with help, and teach them to manage their risk-taking behaviour. Besides the many challenges that young people face, adolescents suffering from BPD can be very vulnerable and difficult to handle [3].
BPD symptoms evolve over time, however, here is a list of a few common symptoms that teenagers face:
One of the best therapies that helps patients to cope with BPD is Dialectical Behavioural Therapy (DBT). This method consists of a cognitive-behavioural approach that emphasises the psycho-social aspects of treatment. DBT is conceived for people that are prone to react in a more intense and out-of-the-ordinary manner toward certain emotional situations, primarily those found in romantic, family and friend relationships [5].
The Monsenso mHealth solution can help clinicians monitor and treat young patients suffering from BPD. In fact, the Mental Health Services in the Region of Southern Denmark (MHS)will soon begin clinical trials of a mobile coach app that supports DBT of BPD patients. To learn more about this project, click here!
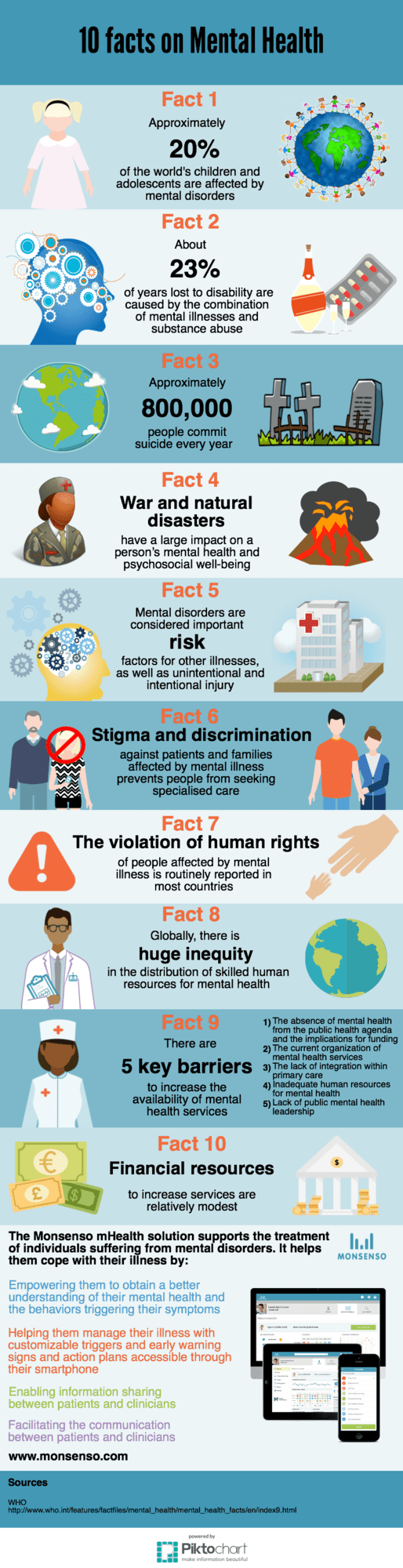
Approximately 20% of the world’s children and adolescents are affected by mental disorders. Mental illnesses and substance abuse are the leading causes of disability worldwide.
Monsenso uses cookies for the purpose of statistical analysis, improving the usability and friendliness of our website, and tailoring content to your interests. By visiting this website, you consent to our and third-party use of cookies as described in our privacy and cookie policy.AcceptRead more