
by Thomas Lethenborg | Dec 8, 2015 | mHealth
Early intervention is critical to treating mental illness before it can cause tragic results such as serious impairment, unemployment, homelessness, poverty, and suicide [1].
The identification of mental illness and its treatment, as early as possible, represents a high priority. The early detection and treatment of mental illness promote recovery, independence, and self-sufficiency, as well as facilitating social activities and employment opportunities [2].
It is estimated that 100,000 adolescents and young adults in the United States alone experience a first episode of psychosis every year. The early phase of psychotic illness is widely viewed as a critical opportunity for indicated prevention, and a chance to alter the downward trajectory and poor outcomes associated with serious mental disorders such as schizophrenia. The timing of treatment is critical; short and long-term outcomes are better when individuals begin treatment close to the onset of psychosis. Numerous studies find a substantial delay between the onset of psychotic symptoms and the initiation of treatment. In the U.S., treatment is typically delayed between one and three years, suggesting that many people experiencing first episodes of psychosis are missing a critical opportunity to benefit from early intervention [3].
Early identification and rapid referral are essential to shortening the duration of untreated psychosis and pre-empting functional deterioration. The World Health Organization advocates reducing the duration of untreated psychosis to three months or less by addressing “bottlenecks” in the pathway from early psychosis identification to initiation of specialty care [3].
To support early intervention, in 2009, the National Institute of Mental Health (NIMH), implemented a research project to change the prognosis of schizophrenia through aggressive treatment in the earliest stages of illness.Recovery After an Initial Schizophrenia Episode (RAISE) is designed to reduce the likelihood of long-term disability that people with schizophrenia often experience. It aims to help people with the disorder lead productive, independent lives. At the same time, it aims to reduce the financial impact on the public systems often tapped to pay for the care of people with schizophrenia [4].
In 2011, RAISE began conducting a full-scale, randomized controlled trial comparing two different ways of providing treatment to people experiencing the early stages of schizophrenia and related disorders. Both types of treatment emphasize early intervention but feature different approaches for initiating and coordinating care. Treatment may include personalized medication treatment, individual resiliency training, and supportive services, such as family psychoeducation and education or employment assistance [5]. The RAISE study, expected to be completed by August 2016, aims to emphasize the importance of early intervention.
The Monsenso mHealth solution can help healthcare providers to closely monitor patients who have experienced a first episode of mental illness.
After experiencing a first episode, the healthcare provider can encourage the patient to use the Monsenso mHealth solution. This will enable the clinician to monitor the individual on a continuous basis, and react if symptoms arise.
With the Monsenso user app, patients can fill in self-assessments on a daily basis. These self-assessments include information on the patient’s behaviour and symptoms related to his mental health. Furthermore, the solution collects sensor data through sensors in the patient’s smartphone, and this combined with the self-assessment will help the healthcare provider to continuously monitor the patient, and support intervention at a very early stage. Early warning signs and automatic triggers can be set to indicate to the health care provider that proactive intervention is needed, if for example a patient sleeps too little or feels too distressed.
Early intervention and continuous monitoring can maximize a person’s chances of a fast recovery, self-sufficiency, and living a high-quality life including the possibility to pursue and education and maintain a stable job.
References:
[1] Directors Blog: SAMHSA and NIMH partner to support early intervention for serious mental illness. P. Hyde and T. Insel. National Institute of Mental Health Blog (2014, June 17) http://www.nimh.nih.gov/about/director/2014/samhsa-and-nimh-partner-to-support-early-intervention-for-serious-mental-illness.shtml
[2] Early intervention and recovery for young people with early psychosis: consensus statement. J. Bertolote and P. McGorry. British Journal of Psychiatry (2005). http://bjp.rcpsych.org/content/bjprcpsych/187/48/s116.full.pdf
[3] Evidence based treatment for first episode of psychosis: Components of coordinated specialty care. PHD R. K. Heinssen. RAISE NIMH (2014, April 14). http://www.nimh.nih.gov/health/topics/schizophrenia/raise/nimh-white-paper-csc-for-fep_147096.pdf
[4] Raise Project Overview. National Institute of Mental Health. (2009)http://www.nimh.nih.gov/health/topics/schizophrenia/raise/index.shtml
[5] NIMH RAISE Project makes progress as team refines research approach. National Institute of Mental Health. (2011, August 9) http://www.nimh.nih.gov/news/science-news/2011/nimh-raise-project-makes-progress-as-teams-refine-research-approaches.shtml

by Thomas Lethenborg | Dec 3, 2015 | Bipolar, mHealth
Bipolar disorder, also known as manic-depressive illness, is a brain disorder that causes unusual shifts in mood, energy, activity levels, and the ability to carry out day-to-day tasks. [1]
People suffering from bipolar disorder will have periods or episodes of depression – where they feel very low and lethargic mania – where they feel high and overactive. [2]
Unlike simple mood swings, each episode of bipolar disorder can last for several weeks and some people may not experience a “normal” mood very often. [2]
Getting an accurate diagnosis is the first step in bipolar disorder treatment. However, this isn’t always easy. The mood swings of bipolar disorder can be difficult to distinguish from other problems such as major depression, ADHD, and borderline personality disorder. For many people suffering from bipolar disorder, it takes years and numerous doctor visits before the problem is correctly identified and treated. [3]
Indicators of bipolar disorder:
- Repeated episodes of major depression
- First episode of major depression was experienced before age 25
- First-degree relative suffering from bipolar disorder
- Mood and energy levels are higher than most people’s when not depressed
- Oversleeping and overeating when depressed
- Episodes of major depression are shorter than 3 months
- Lost contact with reality while depressed
- Suffered from postpartum depression in the past
- Developed mania or hypomania while taking antidepressants
- Antidepressants stopped working after several months
- Tried three or more antidepressants without success [3]
If a person is not treated, episodes of bipolar-related mania can last for between three to six months. Episodes of depression tend to last longer, for between six and twelve months. However, with effective treatment, episodes usually improve within about three months. [2]
Most people with bipolar disorder can be treated using a combination of different treatments that can include:
- Medication such as mood stabilisers and antidepressants
- Learning to recognize triggers and early warning signs of an episode of depression or mania
- Psychotherapy to deal with depression and provide advice on how to improve relationships
- Lifestyle advice such as doing regular exercise, planning activities you enjoy that give you a sense of achievement, and advice on improving your diet and getting more sleep [2]
Mobile health technology
The Monsenso mHealth platform is based on The MONARCA Research Project, aimed at developing and validating a solution for multi-parametric, long-term monitoring of behavioral and physiological information relevant to bipolar disorder.
The Monsenso solution can help predict and prevent episodes by training patients to recognize their early warning signs, which are symptoms that indicate an oncoming episode [4].
In particular, during the research project, it was discovered that these three parameters are crucial in keeping a bipolar patient stable:
- Adherence to prescribed medication: Taking all medications on a daily basis, exactly as prescribed.
- Stable sleep patterns: Sleeping eight hours every night and maintaining a consistent routine of going to bed, waking up.
- Staying active both physically and socially: Getting out of the house every day, going to work, and engaging in social interaction.
Therefore, the Monsenso solution includes five core features that support a patient’s self-management:
- Self-assessments – Reminded by an alarm, patients enter subjective data directly into the system through their smartphones. This data includes mood, sleep, level of activity, and medication. Some items can be customized to accommodate a patient’s specific needs, while others are consistent to provide statistical analysis.
- Activity monitoring – Through a GPS and accelerometer, objective data is collected to monitor a patient’s level of engagement in daily activities. The system can also measure the amount of social activity based on phone calls and text messages.
- Historical overview of data – On the web portal, patients and clinicians can obtain a two-week snapshot of a patient’s basic data for immediate feedback. The portal also gives them access to a detailed historical overview of the data, enabling them to explore it in depth by going back in time, and focusing on specific variables.
- Coaching and self-treatment – The MONARCA systems supported psychotherapy in two ways. Firstly, through customizable triggers that notify the patient and clinician when the data potentially indicates a warning sign. Second, since the patients have access to their own Early Warning Signs, it empowers them to learn more about them.
- Data sharing – To strengthen the relationship between patients and clinicians, important information and treatment decisions are shared.
Resources:
[1] What is bipolar disorder? National Institute of Mental Health. http://www.nimh.nih.gov/health/topics/bipolar-disorder/index.shtml
[2] Bipolar disorder. National Health Service (NHS) UK. http://www.nhs.uk/Conditions/Bipolar-disorder/Pages/Introduction.aspx
[3] Bipolar disorder treatment. HelpGuide.org http://www.helpguide.org/articles/bipolar-disorder/bipolar-disorder-treatment.htm

by Thomas Lethenborg | Nov 19, 2015 | Borderline, mHealth
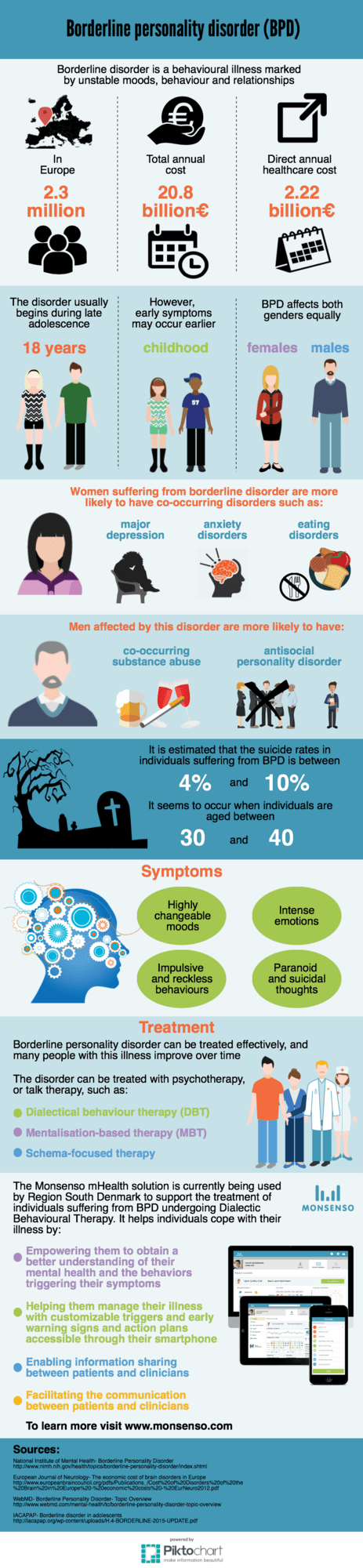
Borderline disorder is a behavioural illness marked by unstable moods, behaviour and relationships.
The disorder usually begins during late adolescence, not before the age of 18 years. However, early symptoms may occur during childhood.

by Thomas Lethenborg | Nov 5, 2015 | Anxiety
To learn more about Anxiety Symptoms click on the link.
by Thomas Lethenborg | Nov 3, 2015 | Anxiety
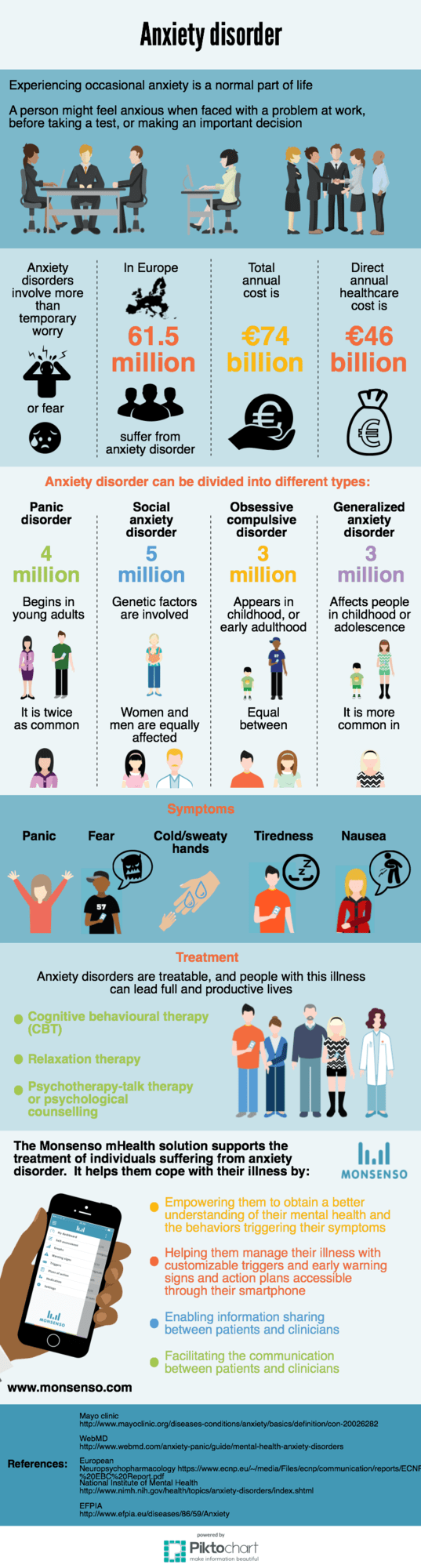
Experiencing occasional anxiety is a normal part of life. However, people with anxiety disorders frequently have intense, excessive and persistent worry and fear about everyday situations. Often, anxiety disorders involve repeated episodes of sudden feelings of intense anxiety and fear or terror that reach a peak within minutes (panic attacks) [1].
Anxiety is the primary symptom of several conditions, including:
- Generalized anxiety disorder (GAD)
- Panic attacks
- Phobias
- Post-traumatic stress disorder
- Social anxiety disorder [2]
- Symptoms of GAD
- Restlessness
- Sense of dread
- Feeling constantly “on edge”
- Difficulty concentrating
- Irritability
- Dizziness
- Tiredness
- Fast or irregular heartbeat
- Muscle aches and tension
- Trembling or shaking
- Shortness of breath
- Headache
- Insomnia [2]
The two main treatments for anxiety disorders are psychotherapy and medication. It is often beneficial to combine both. It may take some trial and error to discover which treatments work best for an individual.
Psychotherapy
Psychotherapy, also known as talk therapy or psychological counselling, involves working with a therapist to reduce a person’s anxiety symptoms. Sometimes, it can be an effective treatment on its own [3].
Cognitive behavioural therapy (CBT) is one of the most effective forms of psychotherapy for anxiety disorders. A short-term treatment, cognitive behavioural therapy focuses on teaching individuals specific skills to return gradually to the situations they avoided due to their anxiety [3].
Applied relaxation focuses on relaxing your muscles in a particular way during situations that usually cause anxiety. The technique needs to be taught by a trained therapist, but involves:
- Learning to relax one’s muscles
- Learning to relax one’s muscles quickly and in response to a trigger, such as the word “relax”
- Relaxing one’s muscles in situations that make a person anxious [2]
Medication
- Antidepressants – this type of medications influences the activity of brain chemicals (neurotransmitters) thought to play a role in anxiety disorders
- Buspirone – an anti-anxiety medication called buspirone may be used on an ongoing basis. As with most antidepressants, it typically takes up to several weeks to become fully effective
- Benzodiazepines – this type of medication are used only for relieving acute anxiety on a short-term basis. Because they can be habit-forming, these medications aren’t a good choice if you’ve had problems with alcohol or drug abuse [1]
The Monsenso mHealth solution for behavioural disorders is currently being used to support the treatment of individuals suffering from bipolar disorder, schizophrenia, depression, and borderline personality disorder.
Although there isn’t any ongoing research on anxiety, it can definitely be used to support the treatment of anxiety with in conjunction with CBT.
Individuals can obtain an overview of their historic levels of anxiety and try to identify the behavioural patterns that trigger their symptoms. Based on their historical records they can learn to predict situations of risk and take preventive measures to avoid or minimize any adverse reactions. Additionally, the Monsenso smartphone app also provides individuals with customized action plans and a secure communication channel with their clinic when they need it the most.
References:
[1] Anxiety. Mayo Clinic.
http://www.mayoclinic.org/diseases-conditions/anxiety/basics/definition/con-20026282
[2] Anxiety. National Institute of Mental Health.
http://www.nimh.nih.gov/health/topics/anxiety-disorders/index.shtml
[3] Anxiety. National Health Service (NHS) UK
http://www.nhs.uk/conditions/anxiety/Pages/Introduction.aspx